.jpg)
.png)
The Science of Seating
Reflections from the 36th International Seating Symposium, 4-6 March 2020
Dr Mark Bowtell
Principal Clinical Scientist, Rehabilitation Engineering, Medical Physics & Clinical Engineering (MPCE), Swansea Bay University Health Board (UHB)
Jacob Redwood-Thomas
Clinical Scientist, Rehabilitation Engineering, MPCE, Swansea Bay UHB
See 1st image:
Mark (left) and Jacob on the Vancouver ski slopes
© Institute of Physics and Engineering in Medicine SCOPE 2020. Reproduced with permission
As the impact of Covid-19 was ramping up at the beginning of March, we braved a trip to Vancouver, Canada, for the 36th International Seating Symposium (ISS). We work in the Special Seating and Pressure Ulcer Prevention and Intervention Service (PUPIS) teams, as part of Rehabilitation Engineering at Swansea Bay University Health Board and went to present, to share knowledge and experience, and to learn from the latest research and equipment advances on that side of the ‘pond’.
INTERNATIONAL SEATING SYMPOSIUM 2020
The conference saw over 1100 therapists, engineers and equipment representatives from 26 countries attend the three and a half day conference. The programme was busy and varied, with themes of aging, obesity, early age mobility, biomechanics, powered assist, posture and function, pressure ulcers and anatomy, dynamic seating, outcome measures, and metadata.
Adventure in powered mobility
One highlight was a conversational plenary session with Dr Lisbeth Nilsson, occupational therapist (OT) from Sweden and Dr Tim Adlam, engineer and educator from England, where they discussed why powered mobility is enabling for children and adults with cognitive disabilities (Durkin 2009). When asked what mobility meant to her, Lisbeth commented ‘Mobility is a key to developmental learning… to explore the world, without limitation’. She went on to say that we often get it wrong in assessment, as we have a culture of being ‘directing’ when we should be prioritising a ‘safe, secure environment to best discover a child’s needs, desires and limitations’.
Lisbeth has spent years campaigning through her research and practice as an OT to provide powered mobility for children below the age of 12. She saw the importance of understanding cause and effect, in being trusted to let go. ‘I don’t call it learning, I call it growing consciousness of the world around us’. ‘Crashing is really important’ she said, and Tim agreed, saying that we should allow our children to fall over because we learn by repetition and failure, and it is the same for those with disabilities. ‘Appropriate boundaries are still important as you wouldn’t let a child fall in a lake, but safety in healthcare can too easily be the antithesis of adventure’. Tim, who has a child with Cerebral Palsy and Autistic Spectrum Condition, concluded ‘We can mitigate risk in later life by allowing appropriate risk in early life’.
Anatomy and pressure ulcers
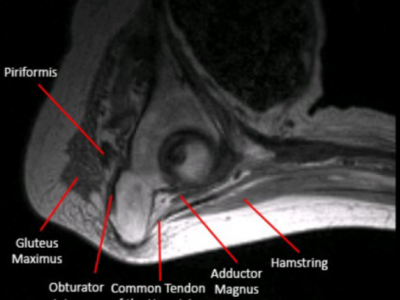
Dr Sharon Sonenblum presented explorations of ischial and coccyx anatomy from seated magnetic resonance imaging (MRI) tests. She compared able-bodies to those with spinal cord injury, for example, commenting on a lack of gluteal maximus coverage underneath the ischial tuberosities for both groups. She also compared the thickness of soft tissue under the ischial tuberosities for different cushions, showing as little as 16mm of compressed soft tissue when sitting on a flat foam cushion, compared to 40mm on a research cushion with ¼ of the surface cut out to intentionally offload the pelvic loading areas. It was also interesting to see how the coccyx differs between people, and how these four vertebra at the base of the spine adopt different postures dependent on sitting position (Sonenblum 2020).
See 2nd image top right:
Seated anatomy under the pelvis and surrounding tissue for a person with a spinal cord injury (Sonenblum 2020) MRI Image © REARLab at Georgia Tech
Dynamic seating
Another session introduced the draft Rehabilitation Engineering and Assistive Technology Society of North America (RESNA) position paper on dynamic seating, opening it up for consultation. The paper defines dynamic seating as:
movement which occurs within the seating system and/or wheelchair frame in response to intentional or unintentional force generated by the client. Dynamic components absorb force, which in turn assists the client back to a starting position (Lange and Crane 2019).
The paper continues to state possible clinical applications of dynamic seating. Clinically, it appears beneficial for patients to be able to express their extensor pattern and return to their original position
whilst minimising risk of injury. Mechanically, the ability of components to absorb forces generated by clients will prolong the components’ lifetime compared to static components. In addition, dynamic seating could be prescribed with the aim of providing sensory input. Finally, such components can improve postural control, stability and function. The following applications are potential benefits of dynamic seating components:
- To protect the wheelchair user from injury
- To protect wheelchair and seating hardware from breakage
- To increase sitting tolerance and compliance
- To enhance vestibular input
- To facilitate active range of motion
- To increase alertness
- To decrease agitation
- To decrease fatigue
- To increase function
- To increase strength and postural control
- To reduce active extension
- To reduce energy consumption
Overall, the talk provided a valuable insight into the progress surrounding a RESNA positioning paper and its contents. The purpose of such papers are to provide advice to healthcare professionals when seating a person, but also to manufacturers and to funding bodies. An area that was not discussed was the possible contraindications of using dynamic seating. This was raised during the discussion, with the presenters stating that contraindications will be added in the ensuing stages.
Rolling Resistance Losses in Manual Wheelchair Propulsion
One interesting study focused on the effect of toe in/out wheel alignment on rolling resistance in manual wheelchair propulsion. Rolling resistance is the force that acts against a user as they manually propel themselves forward. Many shoulder injuries result from self-propelling, and rolling resistance is a major factor (Burnham et al. 1993; Sie et al. 1992). An increase in rolling resistance effectively means that the force required to manually propel is increased. Rolling resistance is the result of energy loss when the tyre deforms and reforms, making the material of the tyre a very important consideration during the prescription process.
The study measured the average change in rolling resistance between 6 different tyres. A test rig showed an average change of 72% of rolling resistance between the best and worst performing tyre, a difference equivalent to carrying an extra 46kg load (Ott et al. 2019). An environmental factor of medium pile carpet was also tested across the six tyres. The next part of study performed a field study looking at toe in/out (malalignment) and slop (play) in wheelchairs being used by the public. Across the 200 participants, the average toe in/out was 0.92° and the average slop was 0.54°, which equates to adding 11kg and 2kg, respectively, to the user’s lap when propelling. Tyre pressure was also analysed. The average tyre pressure was 35% of the maximum, which equates to adding 9kg to the user’s lap. The field study highlighted the importance of issuing the appropriate type of tyre (pneumatic, airless insert, solid); checking for slop or toe angle at review appointments; and educating patients on inflating their tyres and checking for slop.
Why is sitting out important (as opposed to remaining in bed)
- Quality of life – social interaction
- Mental health – goals, routine
- Circulation
- Respiration
- Eating and digestion
- Infection – pneumonia, UTI
- Prevent muscle atrophy & contractures
- Pressure distribution
Note: Sitting up in bed for long periods of time is not a substitute for sitting in appropriately supportive seating. Sacral pressure injury is common in such cases (AWTVNF 2019).
Why is appropriate seating important?
Seating is important in terms of size, set-up, surface and shape (Bowtell 2018; Tasker 2011), for anyone who sits for a period of time without the ability to move or recognise the need to move. Appropriate seating should allow a person to remain supported in a safe, stable and comfortable manner.
The alignment and orientation of the pelvis is paramount, as this will also affect the positioning of the lower limbs and the trunk (Ham et al. 2009). At the seating interface, an estimated 75% of a person’s body weight will pass through the pelvis, with the ischial tuberosities being the main structures of the pelvis in contact with the seat (Collins 2001).
Two common forms of poor sitting posture are ‘sacral sitting’ and ‘lateral asymmetry’. Many develop pressure ulcers over the vulnerable coccyx and/or sacrum, if sat in a slumped position with their pelvis tilted backwards (AWTVNF 2019). Secondly, many develop pressure ulcers under one or other ischial tuberosity due to spinal curvature, pelvic obliquity and/or leaning to one side. Uneven loading of the body can often be avoided by providing appropriate support.
When sitting for any period of time our body looks for positions of least energy expenditure (Pope 2007). Where there is insufficient support, this often results in us adopting postures, which are damaging to the body, whether that be through pressure ulcers developed over hours, or postural asymmetries and limitations developed over weeks and months. To support a person in an upright position and reduce the likelihood of pressure ulcers developing, the aim is to spread their weight evenly over a larger surface area.
See 3rd image top right:
Typical changes in seating posture over time, sacral sitting and asymmetry (Illustrations © Helen Frost & PUPIS)
ISS is joined by other seating symposia around the world including the Nordic, Mediterranean, Oceania and European Seating Symposia.
Thank you to IPEM for travel grant funding, as well as partial bursary from ISS, and support from our local department. The experience did not disappoint, and it confirmed the importance of widening our horizons as professionals. We were able to feed back to the Swansea Rehabilitation Engineering department, with new products and novel processes. We have also gained insight for our clinical practice, whether considerations of how we consider cushions for those with prominent pelvic anatomy, when we consider dynamic seating or how to promote optimal wheelchair set-up.
References
AWTVNF (All Wales Tissue Viability Nurse Forum), PUPIS (Pressure Ulcer Prevention & Intervention Service). All Wales Best Practice Guidelines: Seating and Pressure Ulcers. London: Wounds UK, 2019
Bowtell M (2018) The 4 ‘S’s seating principles to reduce pressure ulcer risk. Available online at https://www.wwic.wales/clinical-partners/pressure-ulcer-prevention-and-intervention-service (Accessed 06.10.2020)
Burnham, R.S., et al., Shoulder pain in wheelchair athletes: the role of muscle imbalance. The American journal of sports medicine, 1993. 21(2): p. 238-242
Collins F (2001) Seating: Educational Booklet. The Wound Care Society 8(1)
Durkin J. Discovering powered mobility skills with children: ‘responsive partners’ in learning. International Journal of Therapy and Rehabilitation. 2009;16(6): 331–341.
Ham R, Aldersea P and Porter D (1998) Wheelchair Users and Postural Seating: A Clinical Approach. New York: Churchill Livingstone
International Standards Organisation (ISO). 2007. ISO 7176: Wheelchairs — Part 26: Vocabulary. [Online] Available at https://www.iso.org/obp/ui/#iso:std:iso:7176:-26:ed-1:v1:en:fig:6 [Accessed: 04.05.2020]
Lange, M. and Crane, B. 2019. A New RESNA Position Paper on Dynamic Seating. Presented at the 36th International Seating Symposium, Vancouver Canada
Pope, P. Severe and Complex Neurological Disability: Management of the Physical Condition. London: Butterworth-Heinemann 2007
Sie, I.H., et al., Upper extremity pain in the post rehabilitation spinal cord injured patient. Archives of physical medicine and rehabilitation, 1992. 73(1): p. 44-48
Sonenblum, S. 2020. Seated Anatomy and Its Impact on Pressure Ulcer Risk. Presented at the 36th International Seating Symposium, Vancouver Canada
Tasker L, H., Shapcott, N. G. and P.M. Holland. The use and validation of a laser scanner for computer aided design and manufacturing of wheelchair seating, Journal of Medical Engineering & Technology. 2011. 35:6-7, pp.377-385





.jpg)



no comments
Add your comment...